Youth Sports
Community Corner: An Open Letter to Volleyball – Amaia Cornute
March 21, 2025
July 19, 2022
Do you know a volleyball player who has back pain with hitting or serving or one dealing with a lower-back bone-stress injury?
When dealing with pain or stress injuries, it would make sense to focus on the lower back area for treatment and relief. However, if you limit that focus to only that one area, you are likely missing an important contributor to back pain.Â
Failing to appreciate the role of shoulder mechanical issues may be a failure to address and treat a primary cause of volleyball back pain. This failure may lead to prolonged pain, time off the court, and reduced performance.Â
Whether you are a junior-level or an Olympic-caliber volleyball player with back pain, chances are that shoulder serving or hitting issues are an important part of the problem.
Let’s work through how serving and hitting shoulder issues can lead to back pain and bone stress injuries.
Starting the serving or hitting motion requires both extension (leaning backward) and rotating the lower back in the direction of ball contact. For a right-handed hitter or server (such as Matt Anderson below), that would mean having the trunk and lower back rotate toward the right.

Finishing a serve or hit requires rotation of the lower back and trunk away from the side of ball contact. Again, for right-handed hitters or servers, such as Jordan Larson, that would mean having the trunk and lower back rotate towards the left after ball contact.

Volleyball bending and rotating movements can put stress on the lumbar vertebrae — the five bones in the lower back between the rib cage and the pelvic bones.
These lumbar vertebrae surround and protect the spinal cord, and certain parts, called the posterior elements, are at unique risk for overload injuries. Repetitive extending and rotating can lead to excessive compression forces on posterior element structures such as the pars interarticularis, pedicles, and articular process/facet joints. The pars interarticularis regions also may have reduced blood supplies during growth spurts, making them even more at risk for overload injuries.Â
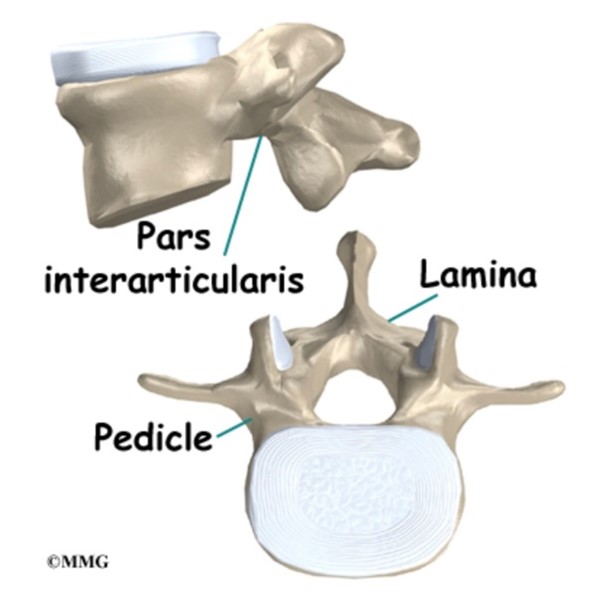
Posterior elements of a lumbar vertebrae, image from https://eorthopod.com/lumbar-spondylolysis/
Injuries to these posterior elements can range from soft tissue overload (such as muscle strains) to bone stress injuries including stress fractures (called spondylolysis in medical terms).Â

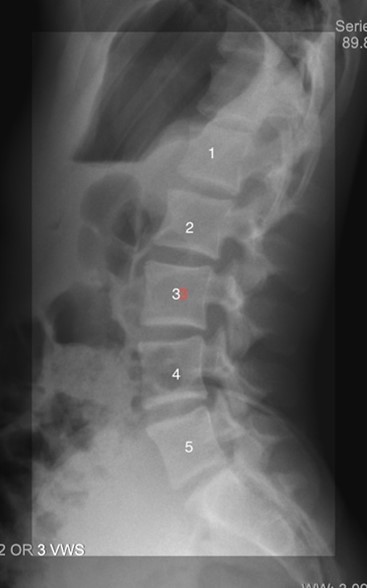
Picture of stress fracture in pars interarticularis of L5 (circled). In this case, the body of L5 has slipped forward due to pars stress fractures on both sides of L5. This condition is called spondylolysis.
CLICK HERE FOR MORE INFORMATION ON BONE STRESS INJURIESÂ
When these types of stress injuries are found, many focus on the lower back as the primary and often only problem area. My experience in working with higher-level volleyball players has taught me that often the dominant shoulder can be a primary contributing culprit to this extension or rotational-based back problem.Â
So now when I evaluate any such type of back pain in a volleyball player, I start by looking at the dominant shoulder.
There are commonly two types of shoulder tightness patterns that can lead to both shoulder problems and pain at the lumbar spine.
PROBLEM ONE: TIGHTNESS OF THE FRONT OF THE SHOULDER AT THE CORACOID PROCESS
The pectoralis minor, coracobrachialis and biceps short head muscles all attach to the coracoid process, which is a bone prominence coming off the scapula. (See Picture Below)
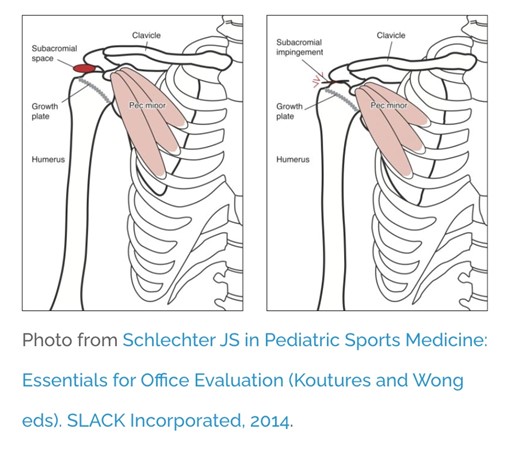
Tightness at this attachment site limits the ability to raise the arm overhead (as in blocking) or getting into the reaching back or “cocked†phase of the early hitting or serving motion. Limitations in reaching back can significantly reduce serving or hitting power.
If a player has limited flexibility at the coracoid, one frequent way to compensate (or some would say, cheat) is to over-rotate the spine towards the hitting/serving shoulder to get the hitting hand far back enough to generate powerful hits or serves.
This over-rotation can at first allow a player to maintain high performance, but ultimately may cause higher cumulative forces on those posterior elements of the lumbar vertebrae and those undesired stress injuries.
This condition causes pain EARLY (before ball contact) in the hitting or serving motions. Tightness in the front of the shoulder often leads to stress injuries on the same side of the lumbar bone as the hitting or serving arm. Proper identification and correction of tightness at the coracoid process can lead to healthier shoulder and back function.
PROBLEM TWO: TIGHTNESS OF POSTERIOR SHOULDER CAPSULE
The glenohumeral joint is the “ball and socket” joint that is surrounded by a soft tissue joint capsule. Repetitive hitting or serving can lead to tightness in the back of this capsule, leading to limitations in shoulder internal rotation or the follow-through phase after ball contact.
Called Glenohumeral Internal Rotation Deficit (GIRD), this tightness can lead to reduced accuracy and speed of hits/serves.
Many volleyball players will compensate (aka cheat) by increasing rotation of the lumbar spine away from the side of the ball after making contact. Eventually, this too will place unwanted forces on those posterior elements of the lumbar vertebrae.
GIRD causes pain LATER (after ball contact) in the hitting or serving motions. Bone stress injuries from GIRD tend to be on the opposite side of the bone from the hitting or serving arm. Just like with anterior shoulder tightness, proper identification and correction of internal rotation limitations can reduce both shoulder and back issues while allowing more high-level function.
CLICK HERE FOR MORE INFORMATION ON VOLLEYBALL SHOULDER TIGHTNESS ISSUES
PRE-EMPTIVE PREVENTION
Don’t wait for the onset of back or shoulder pain to address potential problems. There are quick measurements of both anterior and posterior shoulder motion patterns that can lead to suggestions for stretching programs. Often times your sports medicine physician can routinely incorporate these into pre-season or pre-participation evaluations as part of sensible injury prevention programs.